Description
This research area addresses the theoretical and experimental understanding of motor and balance dysfunction and the effect of disorders on patients in their daily activities.
We develop a wide range of multi-modal assistive tools to support people with neurological movement disorders and psychological disorders. We address the preclinical and clinical phases of various neurological disorders, including Cerebellar Ataxia, Hereditary Spastic Paraplegia, Parkinson’s disease, and Apraxia. Furthermore, multi-modal systems are used to improve therapeutic interventions for mentally ill subjects, e.g., obsessive-compulsive disorders.
Researchers
Abay, Sevinc Nisa; Angehrn, Sarah; Bohn, Kristina; Gehre, Lukas; Ilg, Winfried; Lang, Jana; Laßmann, Christian; Malsch, Milena; Ostertag, Magnus; Salatiello, Alessandro; Seemann, Jens; Thierfelder, Annika; Umer, Syed Muhammad; Willms, Hannah
Current Projects
Real-life gait assessment in degenerative cerebellar ataxia: Towards ecologically valid biomarkers
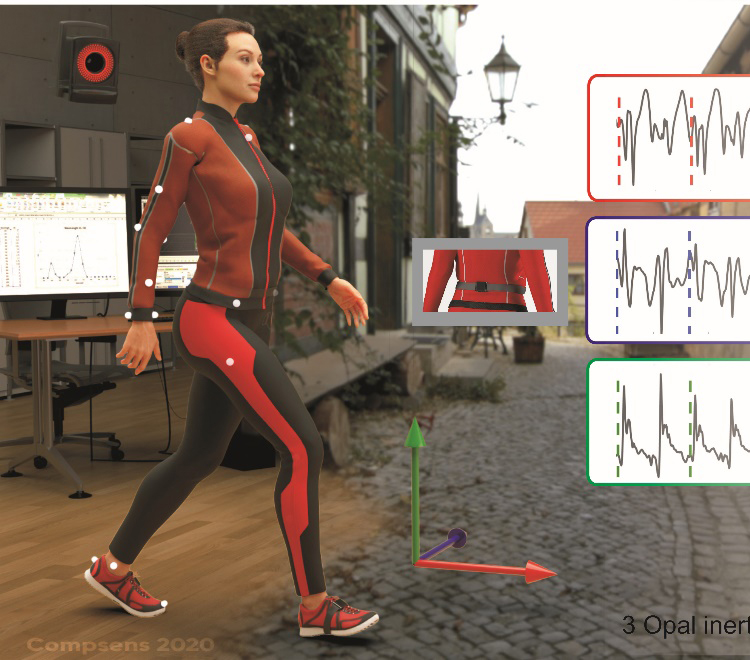
In order to establish ecologically valid biomarkers evaluating treatment-responses really in the patients’ everyday life, we develop multi-variate measures of ataxic gait using wearable sensors, which demonstrate high sensitivity to small differences in disease severity in real-life walking.
Read more
SSTeP KiZ: smart sensor technology in tele-psychotherapy for children and adolescents with obsessive-compulsive disorder
With sensors that can be worn in everyday life and an intelligent analysis of multi-modal sensor data, SSTeP KiZ aims to significantly improve the treatment options for patients with obsessive-compulsive disorder. We support telemedical treatment of affected children and adolescents in their home environment by integrating data collected with wearables.
Read more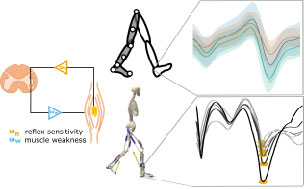
Gait in hereditary spastic paraplegia – from axonal degeneration to movement disorder
In Hereditary Spastic Paraplegia (HSP) type 4 (SPG4 / SPAST) a length-dependent axonal degeneration in the cortico-spinal tract leads to progressing symptoms of hyperreflexia, muscle weakness, and spasticity of lower extremities. The therapeutical potential for future intervention is likely most promising in the early stages of HSP. Therefore, it is crucial to identify and quantify first changes already in the prodromal phase of HSP patients.
Read more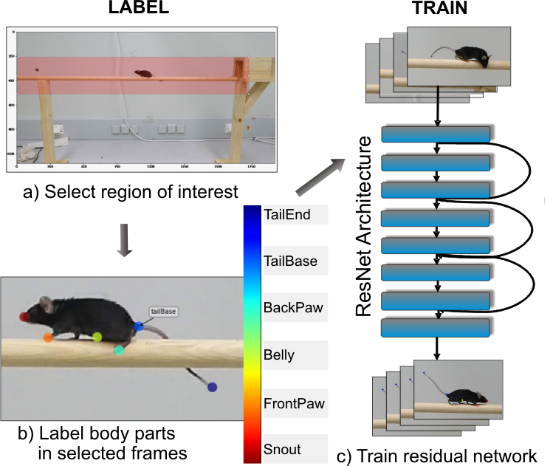
Detecting and Quantifying Ataxia-Related Motor Impairments in Rodents Using Markerless Motion Tracking With Deep Neural Networks
Animal models of adult-onset neurodegenerative diseases have significantly enhanced the understanding of the molecular (patho-)mechanisms and have offered enormous potential for therapeutic target evaluation in many neurodegenerative diseases.
Read moreFinished Projects
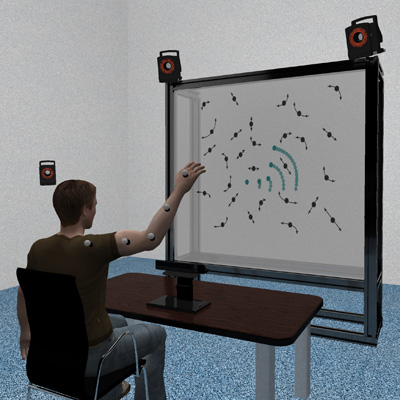
Cerebellar involvement in the facilitation of action perception by concurrent motor activity
The execution of motor behavior influences concurrent visual action observation, and especially the perception of biological motion. Exploiting Virtual Reality technology, we have studied how the cerebellum contributes to action-perception coupling, comparing cerebellar patients with controls.
Read more
Smart sensor technology in telepsychotherapy for children and adolescents SStep-KiZ
Through the use of sensors that can be worn in everyday life and an intelligent analysis of multi-modal sensor data, SSTeP-KiZ aims to significantly improve the treatment options for mentally ill children and adolescents with obsessive-compulsive disorders.
Read more
Development of exergames for the motor training in cerebellar ataxia
Computer games provide a possibility to enhance physiotherapeutic training and to increase the motivation of patients in such training. We develop own games that are optimally adapted to the needs of different patient groups, and specifically cerebellar ataxia patients.
Read more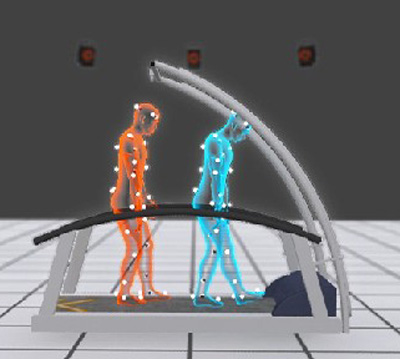
The influence of focal cerebellar lesions on the coordination in walking
In this study we examined patients with focal cerebellar lesions in order to investigate the influence of different regions of the cerebellum on the performance in a working memory task (n-back task), as well as on gait variability and gait stability during dual task walking.
Read more
Cost-efficient system for movement quantification in neurology
The Microsoft Kinect sensor for computer games allows robust body motion tracking for relatively low cost. We use this technology for the analysis of patient movements and develop cheap systems for the quantification of movement deficits that can be deployed at home or simultaneously at multiple places for multi-center studies.
Read more
Design and development of a mobile robot supporting the rehabilitation of free walking
Current walking rehabilitation is mainly restricted to treadmill walking in order to train basic rhythmic walking patterns. Together with the Fraunhofer IPA (Stuttgart) we designed a new robot platform to train walking in complex situations (turning, standing up, etc.).
Read more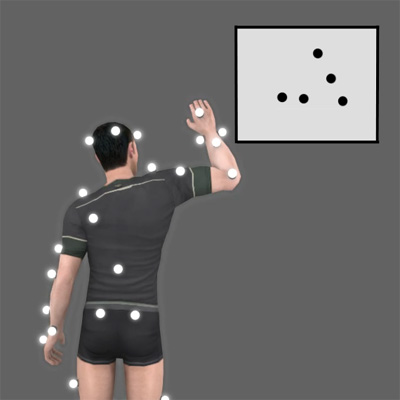
Influence of action execution on biological motion perception
The perception and execution of motor actions are tightly interlinked, and numerous experiments suggest the existence of common sensory-motor representations.Using a virtual-reality setup we aim to investigate the influence of self-generated body motion on the perception of online generated biological motion in combined motor behaviour and psychophysical studies.
Read more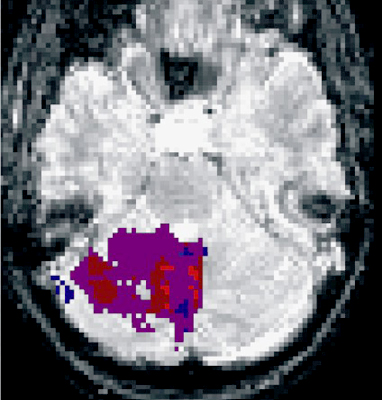
Motor learning and the functional role of the cerebellum
The cerebellum plays an essential role in motor learning. Combining psychophysics and neuropsychological studies in patients we investigate different types of motor learning mechanisms and the role of the cerebellum.
Read more
Quantification of subtle motor changes in preclinical stages of neurodegenerative diseases
Movement disorders such as cerebellar ataxia or Parkinon’s disease result in subtle degradations of motor behavior already long time before the become clinically manifest. Using motion capture technology and machine learning, we try to identify such subtle preclinical motor symptoms.
Read more
Rehabilitation training exploiting physiotherapy, computer games and biofeedback
The symptoms o movement disorders, such as cerebellar ataxia or Parkinon’s disease, can be partially improved y motor training. We have shown that (opposed to the classical view) physiotherapy results in substantial and enduring benefits for patients with cerebellar ataxia, if such training is continuously administered. We exploit biofeedback and computer games to improve such training.
Read morePublications
Gaus, J. A., Ilg, W. & Haeufle, D. (2026). When to Act: Calibrated Confidence for Reliable Human Intention Prediction in Assistive Robotics. arXiv.
More
When to Act: Calibrated Confidence for Reliable Human Intention Prediction in Assistive Robotics
Abstract:
Assistive devices must determine both what a user intends to do and how reliable that prediction is before providing support. We introduce a safety–critical triggering framework based on calibrated probabilities for multimodal next–action prediction in Activities of Daily Living. Raw model confidence often fails to reflect true correctness, posing a safety risk. Post–hoc calibration aligns predicted confidence with empirical reliability and reduces miscalibration by about an order of magnitude without affecting accuracy. The calibrated confidence drives a simple ACT/HOLD rule that acts only when reliability is high and withholds assistance otherwise. This turns the confidence threshold into a quantitative safety parameter for assisted actions and enables verifiable behavior in an assistive control loop
Authors:
Gaus, Johannes A. Ilg, Winfried Haeufle, Daniel
Type of Publication:
Article
Journal:
arXiv
Year:
2026
Full text: PDF | Online version
Willemse, I. H., Mellone, S., Tacconi, C., Ilg, W., Santorelli, F. M., Ricca, I. et al. (2026). Feasibility of a smartphone application for remote use in spastic ataxias: an 8‑week long‑term PROSPAX study. J Neurol, 273.
More
Feasibility of a smartphone application for remote use in spastic ataxias: an 8‑week long‑term PROSPAX study
Authors:
Willemse, Ilse H. J. Mellone, Sabato Tacconi, Carlo Ilg, Winfried Santorelli, Filippo M. Ricca, Ivana Satolli, Sara Klebe, Stephan Jeschonneck, Nicole Schüle, Rebecca Synofzik, Matthis Nonnekes, Jorik van de Warrenburg, Bart P. C.
Type of Publication:
Article
Full text: PDF | Online version
Ilg, W. & Milne, S. (2025). Should Patients Suffering from Degenerative Cerebellar Ataxia Switch from Balance Training to Aerobic Exercise?. Movement Disorders Clinical Practice, n/a-n/a.
More
Should Patients Suffering from Degenerative Cerebellar Ataxia Switch from Balance Training to Aerobic Exercise?
Authors:
Ilg, Winfried; Milne, Sarah
Type of Publication:
Article
Hermle, D., Schubert, R., Barallon, P., Ilg, W., Schüle, R., Reilmann, R. et al. (2025). Digital Outcomes of Upper Limb Ataxia Capture Meaningful Longitudinal Change and Treatment Response. Movement Disorders, n/a(n/a).
More
Digital Outcomes of Upper Limb Ataxia Capture Meaningful Longitudinal Change and Treatment Response
Abstract:
Abstract Background Digital-motor outcomes promise better responsiveness than clinician-reported outcomes in ataxia trials. However, their patient meaningfulness and sensitivity to change remain to be demonstrated, particularly in the upper limb domain. Objectives Validation of quantitative motor (Q-Motor) assessment for upper limb ataxia against patient-reported outcomes and regarding sensitivity to both longitudinal and treatment-induced change, the latter in n-of-1 treatment settings. Methods Single-center longitudinal assessment of finger tapping, diadochokinesia, grip-lift, spiral drawing, and target reaching in (1) 36 cross-genotype ataxia patients and 20 controls, validating digital measures for correlations with patient-reported outcome measure (PROM)-ataxia, 2-weeks test–retest reliability, and sensitivity to change within a trial-relevant 1-year follow-up, anchored in Patient Global Impression of Change (PGI-C); and (2) two patients with spinocerebellar ataxia type 27B (SCA27B) on versus off treatment with 4-aminopyridine. Results Twenty-four digital measures correlated with the PROM-ataxia upper-limb composite (|ρ| = 0.4–0.7) and had excellent test–retest reliability (ICC = 0.91–0.99). Correlations to individual PROM-ataxia items were specific for functional impairment the respective measure was hypothesized to capture. Speed of finger tapping and diadochokinesia, and smoothness of target reaching (spectral arc length of movement in three dimensions [SPARC3D]) captured 1-year progression in ataxia patients (|rprb| = 0.38–0.51), and specifically in patients with worsening PGI-C. Estimated sample sizes to detect longitudinal change were lower for digital than clinical outcomes (SPARC3D: n = 33, Scale for the Assessment and Rating of Ataxia (SARA): n = 79, nine-hole peg-test: n = 214). Speed of diadochokinesia, stability of grip-lift, and variability of target reaching captured treatment responses to 4-aminopyridine in SCA27B, exceeding minimal detectable and minimal important change. Conclusion Digital upper limb measures capture patient-meaningful 1-year longitudinal and treatment-induced change, and are therefore promising outcomes for upcoming ataxia trials. © 2025 The Author(s). Movement Disorders published by Wiley Periodicals LLC on behalf of International Parkinson and Movement Disorder Society.
Authors:
Hermle, Dominik Schubert, Robin Barallon, Pascal Ilg, Winfried; Schüle, Rebecca Reilmann, Ralf Synofzik, Matthis Traschütz, Andreas
Type of Publication:
Article
Full text: PDF | Online version
Bohn, K., Seemann, J., Synofzik, M. & Ilg, W (2025). Turns increase the impact of impaired eye movements on locomotion in cerebellar ataxia. International Society of Posture and Gait Research (ISPGR) Maastricht .
More
Turns increase the impact of impaired eye movements on locomotion in cerebellar ataxia
Abstract:
BACKGROUND AND AIM: Turning movements are a highly relevant component of everyday walking behavior, since 35-45\% of steps are taken during turning. Turning movements are thought to be more challenging in terms of dynamic balance than straight walking, as they require more anticipatory postural adjustments and trunk-limb coordination strategies. In addition, certain types of degenerative cerebellar ataxias are associated with disturbances in eye movements such as nystagmus and disturbed VOR reflexes, which occur particularly during head rotation and peripheral gaze and may therefore affect turning more than straight walking. In this study, we compared the turning movements of SCA27B ataxia patients with downbeat nystagmus (DBN) to those of patients with spinocerebellar ataxia (SCA, types 1, 2, 3, 6) without nystagmus and investigated the influence of the drug 4-aminopyridine (4AP) on the reduction of DBN during turning movements. METHODS: We performed a cross-sectional analysis of motion data collected by three body-worn inertial sensors from subjects with SCA1, 2, 3, 6 (n = 359, SARA = 6.81) as well as SCA27B (n = 49, SARA = 7.0) in two conditions: a) lab-based supervised walking of a 60m corridor at preferred speed, b) lab-based turn task, i.e., subjects were instructed to walk along a T-junction of a corridor, including several 90° turns. Turning analysis included standard measures (i.e., mean and peak angular velocity (MAV, PAV), turn duration (TD), number of steps during turning (NoS)) and a measure quantifying dynamic balance during turning (lateral velocity change, LVC), which has been shown to be sensitive to ataxic-specific changes in turning and has strong correlations with self-reported balance confidence as measured by the ABC score. RESULTS: Turn analysis of the LVC revealed significantly greater impairments during lab-based 90° turning (p = 0.001, Cliff’s δ = 0.45) in SCA27B patients with DBN (n = 18) than in SCA1/2/3/6 patients without oculomotor impairment (n = 359). Small or no effects were found for the standard turn parameters (e.g., PAV (p = 0.49, δ = 0.10), TD (p = 0.30, δ = -0.15). Single-subject analysis of a 4AP-treated SCA27B patient with prominent DBN at right and left gaze directions showed both a reduction in DBN and LVC in the ON treatment phase compared to pre-treatment. The slow phase velocity was reduced by 16.1\% in right and by 51.2\% in left gaze. Accordingly, the LVC decreased by -0.46 m/s (-85.3\%) during right and by -0.51 m/s (-98.38\%) during left turns. Here, no improvements were found for the standard turn parameters. CONCLUSIONS: Ataxia-related oculomotor impairments may increase abnormalities in dynamic balance control during turning, which are not reflected in common compensatory strategies such as slowing down and taking smaller steps. The 4AP-induced reduction in DBN in SCA27B patients improves turning performance, with potentially beneficial implications for everyday walking behavior.
Type of Publication:
In Collection
JRESEARCH_BOOK_TITLE:
International Society of Posture and Gait Research (ISPGR) Maastricht